Hospitals are stuck in a deadly doom loop
They never recovered from covid-19

The diagnosis is simple: “Our health-care system broke in 2020,” says Dr Tom Dolphin, an anaesthetist in London and boss of the British Medical Association. “We like to pretend it didn’t, but it really did.” In the early months of 2020, hospitals paused normal activity to free up beds as they braced for a wave of covid-19 patients. The strategy helped in a moment of crisis. But, several years on, it is becoming clear that those measures did lasting damage to health-care systems. Understanding why is less straightforward.
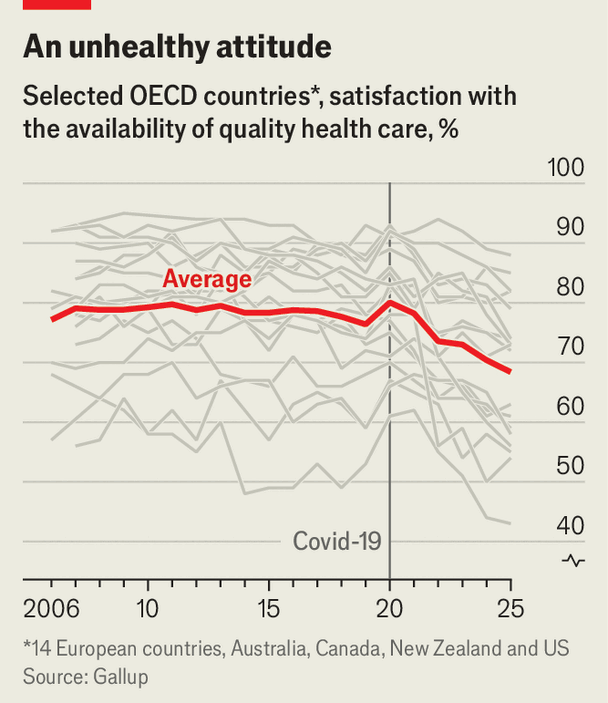
From admission to discharge, hospital care is now harder to access, takes longer and is of worse quality. The resulting toll includes avoidable deaths. Almost everyone is affected: across 18 rich democracies, satisfaction with health-care quality fell sharply after the pandemic and remains well below the pre-pandemic norm (see chart). Few data sets track hospital performance across countries, so The Economist collected data on health-care systems from all over the world to identify where things are going awry.
The ordeal begins outside the emergency room, or the accident-and-emergency department (A&E). Waiting times have become longer in America, Europe and elsewhere. Hospital entry halls are more crowded and their staff more overstretched than they were before the pandemic, says Dr Alex Janke, an emergency physician at the University of Michigan.
In some parts of Australia almost half of patients arriving by ambulance wait more than 30 minutes outside A&E before space can be found for them. About a quarter of patients experience such delays in Britain, double the level in 2019. In Canada a record number of sick and injured simply give up and leave emergency rooms before they are seen by staff.
Once in A&E, care is slow. More than a quarter of patients in England spend over four hours there, roughly twice the level in 2019. In Massachusetts, a state with good data, more than two in five endure such waits. In Australia, nearly half of patients do so. There has also been a steep rise in “trolley waits”, the time between a doctor’s decision to admit a patient from A&E to the hospital and when a patient gets a bed. Last year nearly one in ten emergency admissions in England, or some 550,000 people, had waited more than 12 hours on a trolley—a 67-fold increase since 2019.
The real trolley problem
The Royal College of Emergency Medicine estimates that trolley waits contributed to almost 5,000 avoidable deaths in Britain’s hospitals last summer (health authorities have disputed such figures in the past).
Millions are stuck on waiting lists. Waits for hip replacements, to take one example, were above pre-pandemic levels in 2024 in nine out of 11 OECD countries, for which data exist. Canada is perhaps the worst hit. The median waiting time for specialist treatment was 29 weeks in 2025, more than a third higher than the 2019 baseline, according to the Fraser Institute, a think-tank in Vancouver. That is the second-worst result since the survey began in 1993; the record of 30 weeks was set in 2024. France’s main hospital union says access to health care in the country is undergoing an “unprecedented deterioration”.
In many countries the challenges of hospitals are viewed as the product of domestic policy choices. Britain’s government, like Giorgia Meloni’s in Italy, was elected in part on a promise to reduce waiting lists; Australian voters have punished politicians for ambulances delayed outside A&E; and in France, where staffing shortages have forced the closure of some clinics, there is talk of déserts médicaux.
But the long-term effects of the pandemic on hospitals are consistent across countries. A paper published in January by Luigi Siciliani of the University of York and his co-authors finds no relationship between a health-care system’s characteristics, be it public or private, and the effect of covid on its function. How much funding a system had, its bed capacity and how many physicians it employed, had little to no relation with big jumps in waiting lists for elective surgeries between 2020 and 2023, which occurred across the board.
Hospitals are jammed up despite being well-resourced. Funding for health care is the highest it has ever been, outside covid. After stabilising in the 2010s, spending in the OECD rose to nearly 10% of GDP following the pandemic. Median spending per person in Europe has risen 13% in constant prices since 2019. There are also more helping hands. Hospitals added nearly 140,000 jobs in America last year, more than the entire rest of the economy. Hiring by England’s National Health Service has increased sharply: its headcount has grown by 25% since 2019 to employ some 1.4m people—or 2% of the population.
All this presents a productivity puzzle. Some hospitals seem to be faring worse with more resources. In Australia, where the hospital workforce grew by almost 20% from 2019-24, elective surgeries are basically flat—the only difference is that the sick are waiting longer to be seen. Though there has been a gradual recovery, “On any measure you want to use in England, productivity is below where it was pre-pandemic,” says Max Warner of the Institute for Fiscal Studies, a think-tank in London.
Hospital productivity is hard to measure, but a good rule of thumb for spotting any decline in productivity is when spending grows faster than output, or revenue. Even in Germany, where the public system is considered to be in good shape, three out of four hospitals lost money in 2024, up from a third in 2019, according to a recent report by Roland Berger, a consultancy. In America operating costs for hospitals increased by 7.5% in 2025, about twice as fast as prices, says Aaron Wesolowski of the American Hospital Association, an industry body. Accordingly operating-profit margins have stagnated since 2019, even as profits in the rest of America’s economy recovered and grew.
Experts differ on the reasons why hospitals, as big, complex systems, have never fully recovered. One explanation lies in the hospital workforce. About half of the growth last year in the operating expenses of American hospitals came from inputs such as labour costs, which grew by 5.6% in nominal terms. Pandemic-era stresses increased churn as doctors and nurses resigned, or retired early. Those who stayed have reduced their “discretionary effort”, voluntary overtime work that helped frail health-care systems surge in peak periods. Burnout remains high, says Dr Margot Burnell of the Canadian Medical Association.
Is there a manager in the house?
Both factors have created an acute need for staff, and spurred a big hiring drive. The knock-on effect is that health-care workers today are less experienced and perhaps less productive. In Britain the share of nurses with less than one year of experience has doubled since 2015, a trend explained also by efforts to improve nurse-to-patient ratios. Moreover, though doctors and nurses have been added quickly, in some countries hiring for other jobs vital to productivity, such as theatre assistants and hospital managers, has not kept pace.
The other half of rapidly rising costs comes from having more, and sicker, patients. Four factors apply across rich countries: longer waits have left patients sicker, sicker patients take longer to treat, longer treatments clog capacity, reduced capacity creates longer waits. It is a doom loop.
First, in many places the queue has never been longer. Across the OECD, a group of mostly rich countries, elective-surgery activity dipped in 2020 by 19%. This has left hospitals with a long to-do list on top of their ordinary flow of new patients. More than 3m missed hospital stays accumulated in France between 2019 and 2024, according to estimates by the country’s health-care unions. In January nearly 40% of those waiting for treatment in Britain—or 2.8m people—had been languishing for more than 18 weeks. That was up from 570,000 in the same month of 2019. Mr Siciliani says that in order to cut those lists, hospitals need not only to return to their pre-pandemic productivity, but also to “support a big surge in activity”.
That task is made harder by a second big change: patients are sicker now. Long waits for treatment have made patients’ conditions more complex. Some diseases, such as cancers, stayed undiagnosed for longer because people avoided hospitals and clinics during the pandemic. (In America this effect was compounded by a rising avoidance of treatment due to expense.) In addition, populations are older than they were a few years ago. All this has seen chronic conditions, such as heart disease, cancer and liver disease rise as a share of hospital workloads. Death rates, not adjusted for age, are higher than before the pandemic. “Patients are staying longer and cost more to treat,” says Dr Richard Leuchter, an acute-medicine specialist at the University of California, Los Angeles.
Patients who stay longer take up precious bed capacity. Bed occupancy is further inflated by poorly performing general-practitioner services and chock-full care homes for the elderly, both of which funnel a growing number of sick and infirm into hospitals. Research by Dr Leuchter shows that prior to the pandemic about 64% of American hospital beds were occupied at any given time; during the pandemic that figure shot up to and remained at 75%. In some states, the average is as high as 88% (85% is considered “safe”).
American hospitals look positively capacious next to public systems, which run much leaner. In Ireland more than 94% of beds were occupied in 2019; that went up to 96% in 2025. In Britain beds are often 90% occupied and delays in discharging patients have grown. That worsens the initial problem, delays at the A&E door.
Hospitals are trying to break free from the cycle. Many are demanding more money and staff. A few are trying novel approaches to make room for the sickest patients. Some American hospitals, such as Dr Leuchter’s, are trying “avoidance” strategies that refer stable A&E patients to clinics without overnight beds. Many countries are trying types of “community care” in which treatment occurs outside hospitals, sometimes in patients’ homes. In ageing societies, it was inevitable that hospital care would change: there would be relatively fewer nails in thumbs, and relatively more chronically ill. The pandemic simply made people sicker, sooner. ■